3. The Brain and Spinal Cord
The brain and the spinal cord are the central nervous system, and they represent the main organs of the nervous system. The spinal cord is a single structure, whereas the adult brain is described in terms of four major regions: the cerebrum, the diencephalon, the brain stem, and the cerebellum. A person’s conscious experiences are based on neural activity in the brain. The regulation of homeostasis is governed by a specialized region in the brain. The coordination of reflexes depends on the integration of sensory and motor pathways in the spinal cord.
The Cerebrum
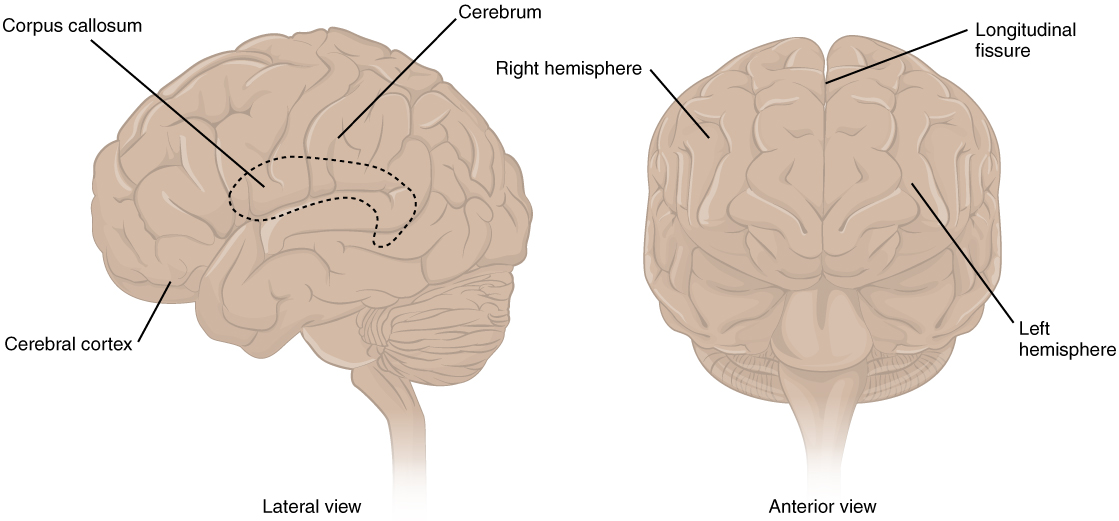
The iconic gray mantle of the human brain, which appears to make up most of the mass of the brain, is the cerebrum (Figure 3.1). The wrinkled portion is the cerebral cortex, and the rest of the structure is beneath that outer covering. There is a large separation between the two sides of the cerebrum called the longitudinal fissure. It separates the cerebrum into two distinct halves, a right and left cerebral hemisphere. Deep within the cerebrum, the white matter of the corpus callosum provides the major pathway for communication between the two hemispheres of the cerebral cortex.
Many of the higher neurological functions, such as memory, emotion, and consciousness, are the result of cerebral function. The complexity of the cerebrum is different across vertebrate species. The cerebrum of the most primitive vertebrates is not much more than the connection for the sense of smell. In mammals, the cerebrum comprises the outer gray matter that is the cortex (from the Latin word meaning “bark of a tree”) and several deep nuclei that belong to three important functional groups. The basal nuclei are responsible for cognitive processing, the most important function being that associated with planning movements. The basal forebrain contains nuclei that are important in learning and memory. The limbic cortex is the region of the cerebral cortex that is part of the limbic system, a collection of structures involved in emotion, memory, and behavior.
Cerebral Cortex
The cerebrum is covered by a continuous layer of gray matter that wraps around either side of the forebrain—the cerebral cortex. This thin, extensive region of wrinkled gray matter is responsible for the higher functions of the nervous system. A gyrus (plural = gyri) is the ridge of one of those wrinkles, and a sulcus (plural = sulci) is the groove between two gyri. The pattern of these folds of tissue indicates specific regions of the cerebral cortex.
The head is limited by the size of the birth canal, and the brain must fit inside the cranial cavity of the skull. Extensive folding in the cerebral cortex enables more gray matter to fit into this limited space. If the gray matter of the cortex were peeled off of the cerebrum and laid out flat, its surface area would be roughly equal to one square meter.
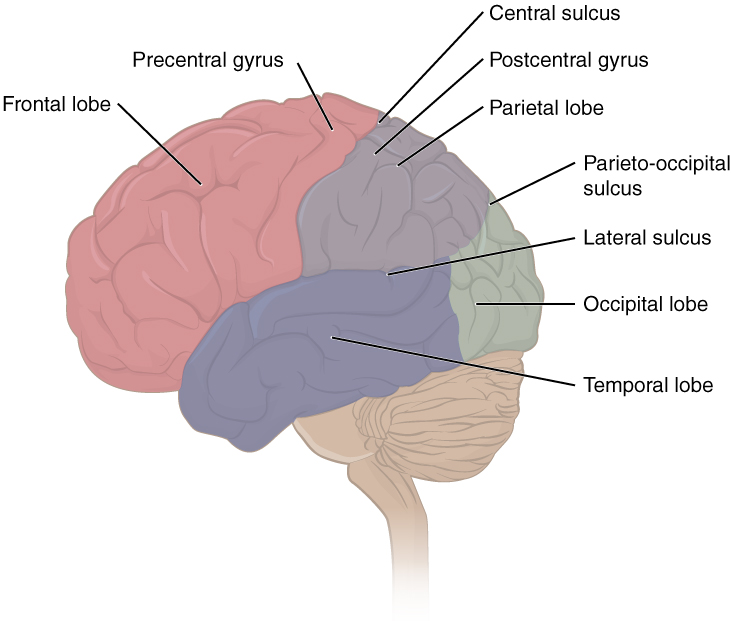
The folding of the cortex maximizes the amount of gray matter in the cranial cavity. During embryonic development, as the telencephalon expands within the skull, the brain goes through a regular course of growth that results in everyone’s brain having a similar pattern of folds. The surface of the brain can be mapped on the basis of the locations of large gyri and sulci. Using these landmarks, the cortex can be separated into four major regions, or lobes (Figure 3.2). The lateral sulcus that separates the temporal lobe from the other regions is one such landmark. Superior to the lateral sulcus are the parietal lobe and frontal lobe, which are separated from each other by the central sulcus. The posterior region of the cortex is the occipital lobe, which has no obvious anatomical border between it and the parietal or temporal lobes on the lateral surface of the brain. From the medial surface, an obvious landmark separating the parietal and occipital lobes is called the parieto-occipital sulcus. The fact that there is no obvious anatomical border between these lobes is consistent with the functions of these regions being interrelated.
Different regions of the cerebral cortex can be associated with particular functions, a concept known as localization of function. In the early 1900s, a German neuroscientist named Korbinian Brodmann performed an extensive study of the microscopic anatomy—the cytoarchitecture—of the cerebral cortex and divided the cortex into 52 separate regions on the basis of the histology of the cortex. His work resulted in a system of classification known as Brodmann’s areas, which is still used today to describe the anatomical distinctions within the cortex (Figure 3.3). The results from Brodmann’s work on the anatomy align very well with the functional differences within the cortex. Areas 17 and 18 in the occipital lobe are responsible for primary visual perception. That visual information is complex, so it is processed in the temporal and parietal lobes as well.
The temporal lobe is associated with primary auditory sensation, known as Brodmann’s areas 41 and 42 in the superior temporal lobe. Because regions of the temporal lobe are part of the limbic system, memory is an important function associated with that lobe. Memory is essentially a sensory function; memories are recalled sensations such as the smell of Mom’s baking or the sound of a barking dog. Even memories of movement are really the memory of sensory feedback from those movements, such as stretching muscles or the movement of the skin around a joint. Structures in the temporal lobe are responsible for establishing long-term memory, but the ultimate location of those memories is usually in the region in which the sensory perception was processed.
The main sensation associated with the parietal lobe is somatosensation, meaning the general sensations associated with the body. Posterior to the central sulcus is the postcentral gyrus, the primary somatosensory cortex, which is identified as Brodmann’s areas 1, 2, and 3. All of the tactile senses are processed in this area, including touch, pressure, tickle, pain, itch, and vibration, as well as more general senses of the body such as proprioception and kinesthesia, which are the senses of body position and movement, respectively.
Anterior to the central sulcus is the frontal lobe, which is primarily associated with motor functions. The precentral gyrus is the primary motor cortex. Cells from this region of the cerebral cortex are the upper motor neurons that instruct cells in the spinal cord and brain stem (lower motor neurons) to move skeletal muscles. Anterior to this region are a few areas that are associated with planned movements. The premotor area is responsible for storing learned movement algorithms which are instructions for complex movements. Different algorithms activate the upper motor neurons in the correct sequence when a complex motor activity is performed. The frontal eye fields are important in eliciting scanning eye movements and in attending to visual stimuli. Broca’s area is responsible for the production of language, or controlling movements responsible for speech; in the vast majority of people, it is located only on the left side. Anterior to these regions is the prefrontal lobe, which serves cognitive functions that can be the basis of personality, short-term memory, and consciousness. The prefrontal lobotomy is an outdated mode of treatment for personality disorders (psychiatric conditions) that profoundly affected the personality of the patient.
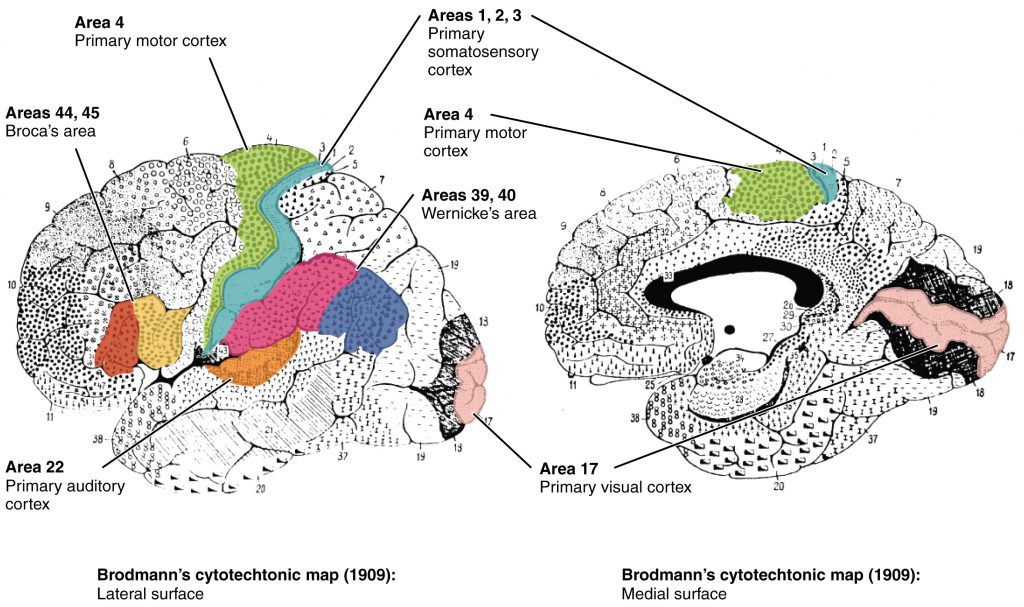
Area 17, as Brodmann described it, is also known as the primary visual cortex. Adjacent to that are areas 18 and 19, which constitute subsequent regions of visual processing. Area 22 is the primary auditory cortex, and it is followed by area 23, which further processes auditory information. Area 4 is the primary motor cortex in the precentral gyrus, whereas area 6 is the premotor cortex. These areas suggest some specialization within the cortex for functional processing, both in sensory and motor regions. The fact that Brodmann’s areas correlate so closely to functional localization in the cerebral cortex demonstrates the strong link between structure and function in these regions.
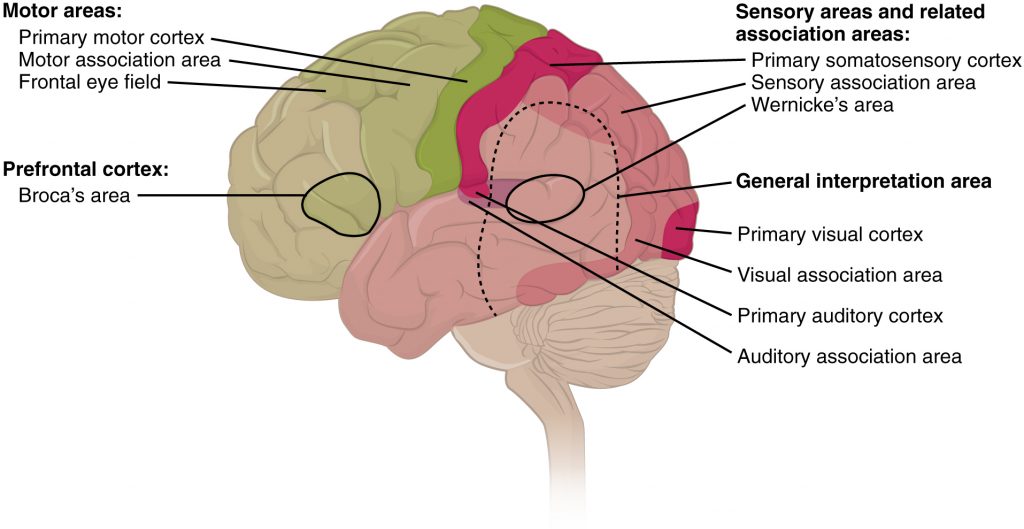
Areas 1, 2, 3, 4, 17, and 22 are each described as primary cortical areas. The adjoining regions are each referred to as association areas. Primary areas are where sensory information is initially received from the thalamus for conscious perception, or—in the case of the primary motor cortex—where descending commands are sent down to the brain stem or spinal cord to execute movements (Figure 3.4).
Functions of the Cerebral Cortex
The cerebrum is the seat of many of the higher mental functions, such as memory and learning, language, and conscious perception, which are the subjects of subtests of the mental status exam. The cerebral cortex is the thin layer of gray matter on the outside of the cerebrum. It is approximately a millimeter thick in most regions and highly folded to fit within the limited space of the cranial vault. These higher functions are distributed across various regions of the cortex, and specific locations can be said to be responsible for particular functions. There is a limited set of regions, for example, that are involved in language function, and they can be subdivided on the basis of the particular part of language function that each governs.
A number of other regions, which extend beyond these primary or association areas of the cortex, are referred to as integrative areas. These areas are found in the spaces between the domains for particular sensory or motor functions, and they integrate multisensory information, or process sensory or motor information in more complex ways. Consider, for example, the posterior parietal cortex that lies between the somatosensory cortex and visual cortex regions. This has been ascribed to the coordination of visual and motor functions, such as reaching to pick up a glass. The somatosensory function that would be part of this is the proprioceptive feedback from moving the arm and hand. The weight of the glass, based on what it contains, will influence how those movements are executed.
Cognitive Abilities
Assessment of cerebral functions is directed at cognitive abilities. The abilities assessed through the mental status exam can be separated into four groups: orientation and memory, language and speech, sensorium, and judgment and abstract reasoning.
Orientation and Memory
Orientation is the patient’s awareness of his or her immediate circumstances. It is awareness of time, not in terms of the clock, but of the date and what is occurring around the patient. It is awareness of place, such that a patient should know where he or she is and why. It is also awareness of who the patient is—recognizing personal identity and being able to relate that to the examiner. The initial tests of orientation are based on the questions, “Do you know what the date is?” or “Do you know where you are?” or “What is your name?” Further understanding of a patient’s awareness of orientation can come from questions that address remote memory, such as “Who is the President of the United States?”, or asking what happened on a specific date.
There are also specific tasks to address memory. One is the three-word recall test. The patient is given three words to recall, such as book, clock, and shovel. After a short interval, during which other parts of the interview continue, the patient is asked to recall the three words. Other tasks that assess memory—aside from those related to orientation—have the patient recite the months of the year in reverse order to avoid the overlearned sequence and focus on the memory of the months in an order, or to spell common words backwards, or to recite a list of numbers back.
Memory is largely a function of the temporal lobe, along with structures beneath the cerebral cortex such as the hippocampus and the amygdala. The storage of memory requires these structures of the medial temporal lobe. A famous case of a man who had both medial temporal lobes removed to treat intractable epilepsy provided insight into the relationship between the structures of the brain and the function of memory.
Henry Molaison, who was referred to as patient HM when he was alive, had epilepsy localized to both of his medial temporal lobes. In 1953, a bilateral lobectomy was performed that alleviated the epilepsy but resulted in the inability for HM to form new memories—a condition called anterograde amnesia. HM was able to recall most events from before his surgery, although there was a partial loss of earlier memories, which is referred to as retrograde amnesia. HM became the subject of extensive studies into how memory works. What he was unable to do was form new memories of what happened to him, what are now called episodic memory. Episodic memory is autobiographical in nature, such as remembering riding a bicycle as a child around the neighborhood, as opposed to the procedural memory of how to ride a bike. HM also retained his short-term memory, such as what is tested by the three-word task described above. After a brief period, those memories would dissipate or decay and not be stored in the long-term because the medial temporal lobe structures were removed.
The difference in short-term, procedural, and episodic memory, as evidenced by patient HM, suggests that there are different parts of the brain responsible for those functions. The long-term storage of episodic memory requires the hippocampus and related medial temporal structures, and the location of those memories is in the multimodal integration areas of the cerebral cortex. However, short-term memory—also called working or active memory—is localized to the prefrontal lobe. Because patient HM had only lost his medial temporal lobe—and lost very little of his previous memories, and did not lose the ability to form new short-term memories—it was concluded that the function of the hippocampus, and adjacent structures in the medial temporal lobe, is to move (or consolidate) short-term memories (in the pre-frontal lobe) to long-term memory (in the temporal lobe).
The prefrontal cortex can also be tested for the ability to organize information. In one subtest of the mental status exam called set generation, the patient is asked to generate a list of words that all start with the same letter, but not to include proper nouns or names. The expectation is that a person can generate such a list of at least 10 words within 1 minute. Many people can likely do this much more quickly, but the standard separates the accepted normal from those with compromised prefrontal cortices.
Language and Speech
Language is, arguably, a very human aspect of neurological function. There are certainly strides being made in understanding communication in other species, but much of what makes the human experience seemingly unique is its basis in language. Any understanding of our species is necessarily reflective, as suggested by the question “What am I?” And the fundamental answer to this question is suggested by the famous quote by René Descartes: “Cogito Ergo Sum” (translated from Latin as “I think, therefore I am”). Formulating an understanding of yourself is largely describing who you are to yourself. It is a confusing topic to delve into, but language is certainly at the core of what it means to be self-aware.
The neurological exam has two specific subtests that address language. One measures the ability of the patient to understand language by asking them to follow a set of instructions to perform an action, such as “touch your right finger to your left elbow and then to your right knee.” Another subtest assesses the fluency and coherency of language by having the patient generate descriptions of objects or scenes depicted in drawings, and by reciting sentences or explaining a written passage. Language, however, is important in so many ways in the neurological exam. The patient needs to know what to do, whether it is as simple as explaining how the knee-jerk reflex is going to be performed, or asking a question such as “What is your name?” Often, language deficits can be determined without specific subtests; if a person cannot reply to a question properly, there may be a problem with the reception of language.
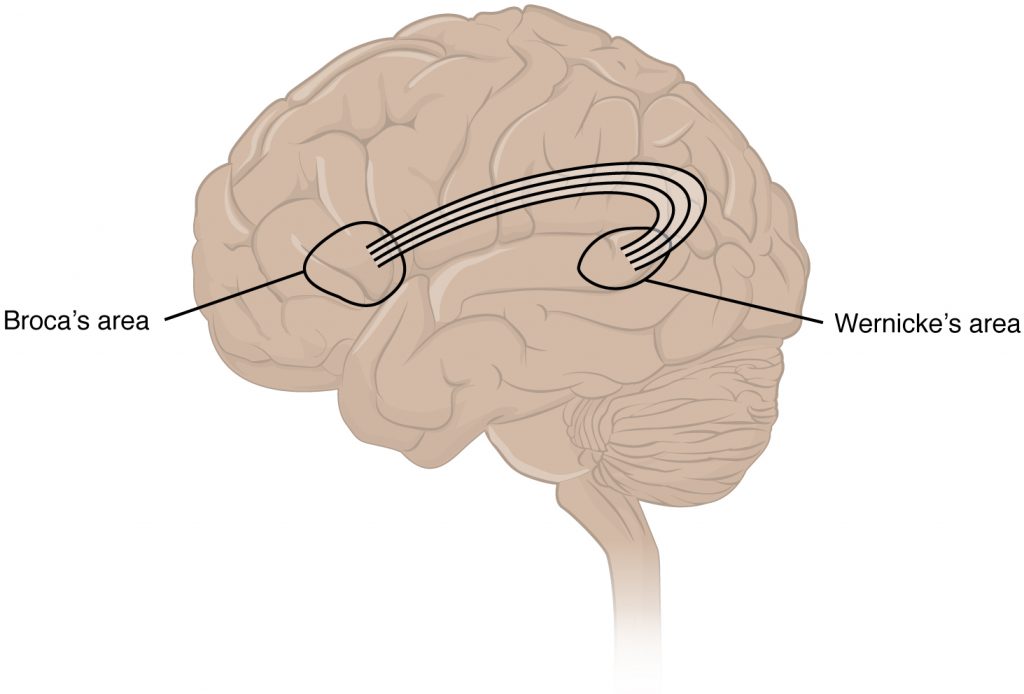
An important example of multimodal integrative areas is associated with language function (Figure 3.5). Adjacent to the auditory association cortex, at the end of the lateral sulcus just anterior to the visual cortex, is Wernicke’s area. In the lateral aspect of the frontal lobe, just anterior to the region of the motor cortex associated with the head and neck, is Broca’s area. Both regions were originally described on the basis of losses of speech and language, which is called aphasia. The aphasia associated with Broca’s area is known as an expressive aphasia, which means that speech production is compromised. This type of aphasia is often described as non-fluency because the ability to say some words leads to broken or halting speech. Grammar can also appear to be lost. The aphasia associated with Wernicke’s area is known as a receptive aphasia, which is not a loss of speech production, but a loss of understanding of content. Patients, after recovering from acute forms of this aphasia, report not being able to understand what is said to them or what they are saying themselves, but they often cannot keep from talking.
The two regions are connected by white matter tracts that run between the posterior temporal lobe and the lateral aspect of the frontal lobe. Conduction aphasia associated with damage to this connection refers to the problem of connecting the understanding of language to the production of speech. This is a very rare condition, but is likely to present as an inability to faithfully repeat spoken language.
Sensorium
Those parts of the brain involved in the reception and interpretation of sensory stimuli are referred to collectively as the sensorium. The cerebral cortex has several regions that are necessary for sensory perception. From the primary cortical areas of the somatosensory, visual, auditory, and gustatory senses to the association areas that process information in these modalities, the cerebral cortex is the seat of conscious sensory perception. In contrast, sensory information can also be processed by deeper brain regions, which we may vaguely describe as subconscious—for instance, we are not constantly aware of the proprioceptive information that the cerebellum uses to maintain balance. Several of the subtests can reveal activity associated with these sensory modalities, such as being able to hear a question or see a picture. Two subtests assess specific functions of these cortical areas.
The first is praxis, a practical exercise in which the patient performs a task completely on the basis of verbal description without any demonstration from the examiner. For example, the patient can be told to take their left hand and place it palm down on their left thigh, then flip it over so the palm is facing up, and then repeat this four times. The examiner describes the activity without any movements on their part to suggest how the movements are to be performed. The patient needs to understand the instructions, transform them into movements, and use sensory feedback, both visual and proprioceptive, to perform the movements correctly.
The second subtest for sensory perception is gnosis, which involves two tasks. The first task, known as stereognosis, involves the naming of objects strictly on the basis of the somatosensory information that comes from manipulating them. The patient keeps their eyes closed and is given a common object, such as a coin, that they have to identify. The patient should be able to indicate the particular type of coin, such as a dime versus a penny, or a nickel versus a quarter, on the basis of the sensory cues involved. For example, the size, thickness, or weight of the coin may be an indication, or to differentiate the pairs of coins suggested here, the smooth or corrugated edge of the coin will correspond to the particular denomination. The second task, graphesthesia, is to recognize numbers or letters written on the palm of the hand with a dull pointer, such as a pen cap.
Praxis and gnosis are related to the conscious perception and cortical processing of sensory information. Being able to transform verbal commands into a sequence of motor responses, or to manipulate and recognize a common object and associate it with a name for that object. Both subtests have language components because language function is integral to these functions. The relationship between the words that describe actions, or the nouns that represent objects, and the cerebral location of these concepts is suggested to be localized to particular cortical areas. Certain aphasias can be characterized by a deficit of verbs or nouns, known as V impairment or N impairment, or may be classified as V–N dissociation. Patients have difficulty using one type of word over the other. To describe what is happening in a photograph as part of the expressive language subtest, a patient will use active- or image-based language. The lack of one or the other of these components of language can relate to the ability to use verbs or nouns. Damage to the region at which the frontal and temporal lobes meet, including the region known as the insula, is associated with V impairment; damage to the middle and inferior temporal lobe is associated with N impairment.
Judgment and Abstract Reasoning
Planning and producing responses requires an ability to make sense of the world around us. Making judgments and reasoning in the abstract are necessary to produce movements as part of larger responses. For example, when your alarm goes off, do you hit the snooze button or jump out of bed? Is 10 extra minutes in bed worth the extra rush to get ready for your day? Will hitting the snooze button multiple times lead to feeling more rested or result in a panic as you run late? How you mentally process these questions can affect your whole day.
The prefrontal cortex is responsible for the functions responsible for planning and making decisions. In the mental status exam, the subtest that assesses judgment and reasoning is directed at three aspects of frontal lobe function. First, the examiner asks questions about problem solving, such as “If you see a house on fire, what would you do?” The patient is also asked to interpret common proverbs, such as “Don’t look a gift horse in the mouth.” Additionally, pairs of words are compared for similarities, such as apple and orange, or lamp and cabinet.
The prefrontal cortex is composed of the regions of the frontal lobe that are not directly related to specific motor functions. The most posterior region of the frontal lobe, the precentral gyrus, is the primary motor cortex. Anterior to that are the premotor cortex, Broca’s area, and the frontal eye fields, which are all related to planning certain types of movements. Anterior to what could be described as motor association areas are the regions of the prefrontal cortex. They are the regions in which judgment, abstract reasoning, and working memory are localized. The antecedents to planning certain movements are judging whether those movements should be made, as in the example of deciding whether to hit the snooze button.
To an extent, the prefrontal cortex may be related to personality. The neurological exam does not necessarily assess personality, but it can be within the realm of neurology or psychiatry. A clinical situation that suggests this link between the prefrontal cortex and personality comes from the story of Phineas Gage, the railroad worker from the mid-1800s who had a metal spike impale his prefrontal cortex. There are suggestions that the steel rod led to changes in his personality. A man who was a quiet, dependable railroad worker became a raucous, irritable drunkard. Later anecdotal evidence from his life suggests that he was able to support himself, although he had to relocate and take on a different career as a stagecoach driver.
A psychiatric practice to deal with various disorders was the prefrontal lobotomy. This procedure was common in the 1940s and early 1950s, until antipsychotic drugs became available. The connections between the prefrontal cortex and other regions of the brain were severed. The disorders associated with this procedure included some aspects of what are now referred to as personality disorders, but also included mood disorders and psychoses. Depictions of lobotomies in popular media suggest a link between cutting the white matter of the prefrontal cortex and changes in a patient’s mood and personality, though this correlation is not well understood.
The Mental Status Exam
The cerebrum, particularly the cerebral cortex, is the location of important cognitive functions that are the focus of the mental status exam. The regionalization of the cortex, initially described on the basis of anatomical evidence of cytoarchitecture, reveals the distribution of functionally distinct areas. Cortical regions can be described as primary sensory or motor areas, association areas, or multimodal integration areas. The functions attributed to these regions include attention, memory, language, speech, sensation, judgment, and abstract reasoning.
The mental status exam addresses these cognitive abilities through a series of subtests designed to elicit particular behaviors ascribed to these functions. The loss of neurological function can illustrate the location of damage to the cerebrum. Memory functions are attributed to the temporal lobe, particularly the medial temporal lobe structures known as the hippocampus and amygdala, along with the adjacent cortex. Evidence of the importance of these structures comes from the side effects of a bilateral temporal lobectomy that were studied in detail in patient HM.
Losses of language and speech functions, known as aphasias, are associated with damage to the important integration areas in the left hemisphere known as Broca’s or Wernicke’s areas, as well as the connections in the white matter between them. Different types of aphasia are named for the particular structures that are damaged. Assessment of the functions of the sensorium includes praxis and gnosis. The subtests related to these functions depend on multimodal integration, as well as language-dependent processing.
The prefrontal cortex contains structures important for planning, judgment, reasoning, and working memory. Damage to these areas can result in changes to personality, mood, and behavior. The famous case of Phineas Gage suggests a role for this cortex in personality, as does the outdated practice of prefrontal lobectomy.
Subcortical structures
Beneath the cerebral cortex are sets of nuclei known as subcortical nuclei that augment cortical processes. The nuclei of the basal forebrain serve as the primary location for acetylcholine production, which modulates the overall activity of the cortex, possibly leading to greater attention to sensory stimuli. Alzheimer’s disease is associated with a loss of neurons in the basal forebrain. The hippocampus and amygdala are medial-lobe structures that, along with the adjacent cortex, are involved in long-term memory formation and emotional responses. The basal nuclei are a set of nuclei in the cerebrum responsible for comparing cortical processing with the general state of activity in the nervous system to influence the likelihood of movement taking place. For example, while a student is sitting in a classroom listening to a lecture, the basal nuclei will keep the urge to jump up and scream from actually happening. (The basal nuclei are also referred to as the basal ganglia, although that is potentially confusing because the term ganglia is typically used for peripheral structures.)
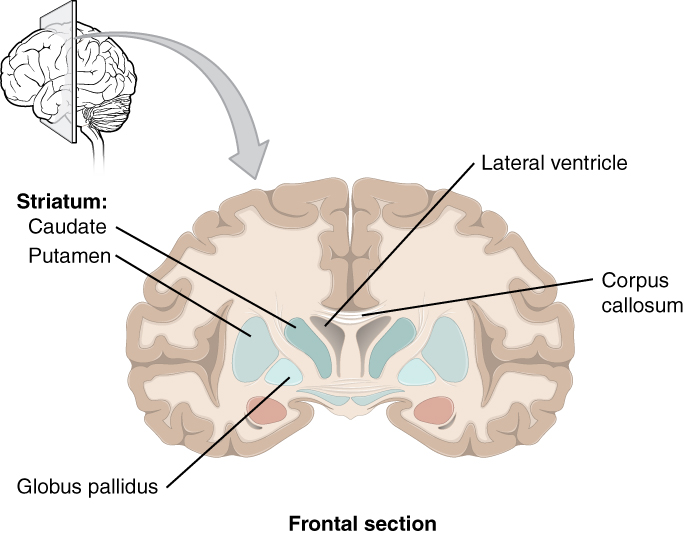
The major structures of the basal nuclei that control movement are the caudate, putamen, and globus pallidus, which are located deep in the cerebrum. The caudate is a long nucleus that follows the basic C-shape of the cerebrum from the frontal lobe, through the parietal and occipital lobes, into the temporal lobe. The putamen is mostly deep in the anterior regions of the frontal and parietal lobes. Together, the caudate and putamen are called the striatum. The globus pallidus is a layered nucleus that lies just medial to the putamen; they are called the lenticular nuclei because they look like curved pieces fitting together like lenses. The globus pallidus has two subdivisions, the external and internal segments, which are lateral and medial, respectively. These nuclei are depicted in a frontal section of the brain in Figure 3.6.
The basal nuclei in the cerebrum are connected with a few more nuclei in the brain stem that together act as a functional group that forms a motor pathway. Two streams of information processing take place in the basal nuclei. All input to the basal nuclei is from the cortex into the striatum (Figure 3.7). The direct pathway is the projection of axons from the striatum to the globus pallidus internal segment (GPi) and the substantia nigra pars reticulata (SNr). The GPi/SNr then projects to the thalamus, which projects back to the cortex. The indirect pathway is the projection of axons from the striatum to the globus pallidus external segment (GPe), then to the subthalamic nucleus (STN), and finally to GPi/SNr. The two streams both target the GPi/SNr, but one has a direct projection and the other goes through a few intervening nuclei. The direct pathway causes the disinhibition of the thalamus (inhibition of one cell on a target cell that then inhibits the first cell), whereas the indirect pathway causes, or reinforces, the normal inhibition of the thalamus. The thalamus then can either excite the cortex (as a result of the direct pathway) or fail to excite the cortex (as a result of the indirect pathway).
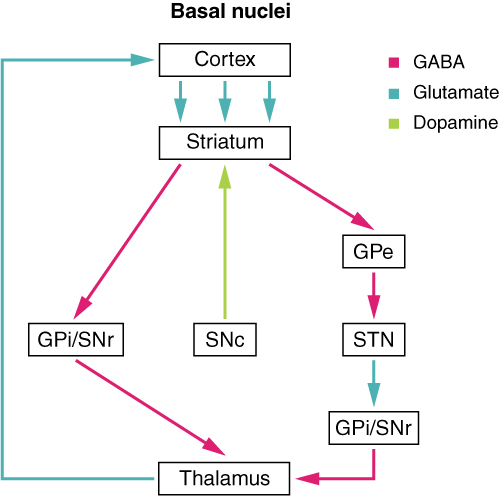
The switch between the two pathways is the substantia nigra pars compacta, which projects to the striatum and releases the neurotransmitter dopamine. Dopamine receptors are either excitatory (D1-type receptors) or inhibitory (D2-type receptors). The direct pathway is activated by dopamine, and the indirect pathway is inhibited by dopamine. When the substantia nigra pars compacta is firing, it signals to the basal nuclei that the body is in an active state, and movement will be more likely. When the substantia nigra pars compacta is silent, the body is in a passive state, and movement is inhibited. To illustrate this situation, while a student is sitting listening to a lecture, the substantia nigra pars compacta would be silent and the student less likely to get up and walk around. Likewise, while the professor is lecturing, and walking around at the front of the classroom, the professor’s substantia nigra pars compacta would be active, in keeping with his or her activity level.
The Diencephalon
The diencephalon is the one region of the adult brain that retains its name from embryologic development. The etymology of the word diencephalon translates to “through brain.” It is the connection between the cerebrum and the rest of the nervous system, with one exception. The rest of the brain, the spinal cord, and the PNS all send information to the cerebrum through the diencephalon. Output from the cerebrum passes through the diencephalon. The single exception is the system associated with olfaction, or the sense of smell, which connects directly with the cerebrum. In the earliest vertebrate species, the cerebrum was not much more than olfactory bulbs that received peripheral information about the chemical environment (to call it smell in these organisms is imprecise because they lived in the ocean).
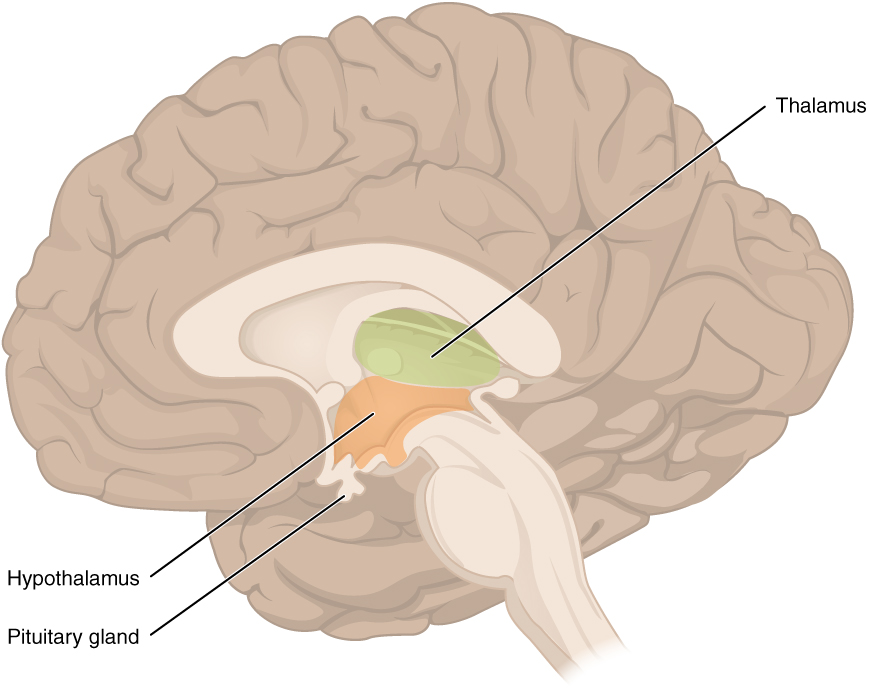
The diencephalon is deep beneath the cerebrum and constitutes the walls of the third ventricle. The diencephalon can be described as any region of the brain with “thalamus” in its name. The two major regions of the diencephalon are the thalamus itself and the hypothalamus (Figure 3.8). There are other structures, such as the epithalamus, which contains the pineal gland, or the subthalamus, which includes the subthalamic nucleus that is part of the basal nuclei.
Thalamus
The thalamus is a collection of nuclei that relay information between the cerebral cortex and the periphery, spinal cord, or brain stem. All sensory information, except for the sense of smell, passes through the thalamus before processing by the cortex. Axons from the peripheral sensory organs, or intermediate nuclei, synapse in the thalamus, and thalamic neurons project directly to the cerebrum. It is a requisite synapse in any sensory pathway, except for olfaction. The thalamus does not just pass the information on, it also processes that information. For example, the portion of the thalamus that receives visual information will influence what visual stimuli are important, or what receives attention.
The cerebrum also sends information down to the thalamus, which usually communicates motor commands. This involves interactions with the cerebellum and other nuclei in the brain stem. The cerebrum interacts with the basal nuclei, which involves connections with the thalamus. The primary output of the basal nuclei is to the thalamus, which relays that output to the cerebral cortex. The cortex also sends information to the thalamus that will then influence the effects of the basal nuclei.
Hypothalamus
Inferior and slightly anterior to the thalamus is the hypothalamus, the other major region of the diencephalon. The hypothalamus is a collection of nuclei that are largely involved in regulating homeostasis. The hypothalamus is the executive region in charge of the autonomic nervous system and the endocrine system through its regulation of the anterior pituitary gland. Other parts of the hypothalamus are involved in memory and emotion as part of the limbic system.
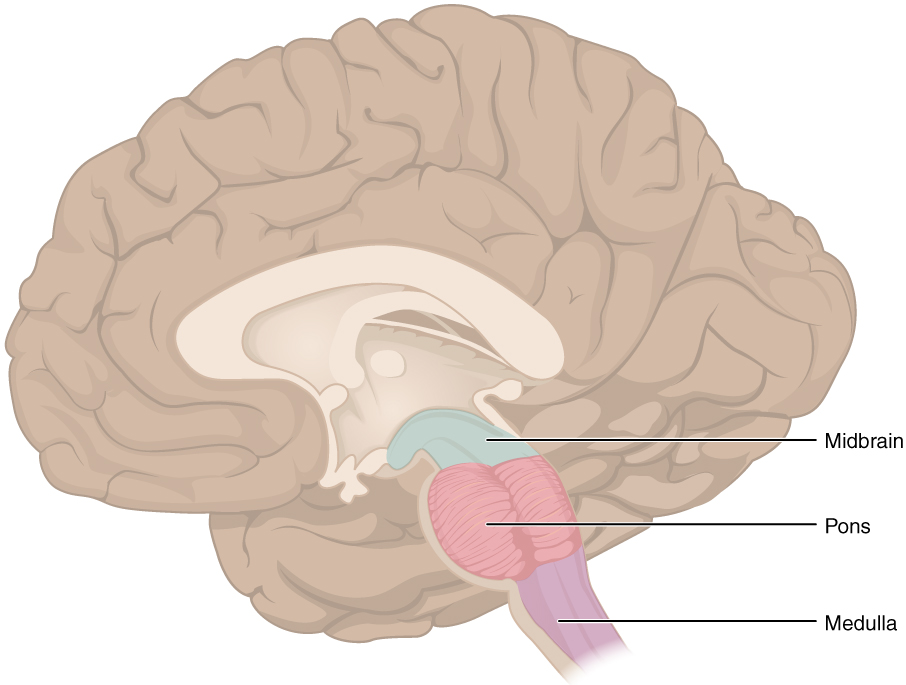
Brain Stem
The midbrain and the pons and medulla of the hindbrain are collectively referred to as the “brain stem” (Figure 3.9). The structure emerges from the ventral surface of the forebrain as a tapering cone that connects the brain to the spinal cord. Attached to the brain stem, but considered a separate region of the adult brain, is the cerebellum. The midbrain coordinates sensory representations of the visual, auditory, and somatosensory perceptual spaces. The pons is the main connection with the cerebellum. The pons and the medulla regulate several crucial functions, including the cardiovascular and respiratory systems.
The cranial nerves connect through the brain stem and provide the brain with the sensory input and motor output associated with the head and neck, including most of the special senses. The major ascending and descending pathways between the spinal cord and brain, specifically the cerebrum, pass through the brain stem.
Midbrain
One of the original regions of the embryonic brain, the midbrain is a small region between the thalamus and pons. It is separated into the tectum and tegmentum, from the Latin words for roof and floor, respectively. The cerebral aqueduct passes through the center of the midbrain, such that these regions are the roof and floor of that canal.
The tectum is composed of four bumps known as the colliculi (singular = colliculus), which means “little hill” in Latin. The inferior colliculus is the inferior pair of these enlargements and is part of the auditory brain stem pathway. Neurons of the inferior colliculus project to the thalamus, which then sends auditory information to the cerebrum for the conscious perception of sound. The superior colliculus is the superior pair and combines sensory information about visual space, auditory space, and somatosensory space. Activity in the superior colliculus is related to orienting the eyes to a sound or touch stimulus. If you are walking along the sidewalk on campus and you hear chirping, the superior colliculus coordinates that information with your awareness of the visual location of the tree right above you. That is the correlation of auditory and visual maps. If you suddenly feel something wet fall on your head, your superior colliculus integrates that with the auditory and visual maps and you know that the chirping bird just relieved itself on you. You want to look up to see the culprit, but do not.
The tegmentum is continuous with the gray matter of the rest of the brain stem. Throughout the midbrain, pons, and medulla, the tegmentum contains the nuclei that receive and send information through the cranial nerves, as well as regions that regulate important functions such as those of the cardiovascular and respiratory systems.
Pons
The word pons comes from the Latin word for bridge. It is visible on the anterior surface of the brain stem as the thick bundle of white matter attached to the cerebellum. The pons is the main connection between the cerebellum and the brain stem. The bridge-like white matter is only the anterior surface of the pons; the gray matter beneath that is a continuation of the tegmentum from the midbrain. Gray matter in the tegmentum region of the pons contains neurons receiving descending input from the forebrain that is sent to the cerebellum.
Medulla
The medulla is the region known as the myelencephalon in the embryonic brain. The initial portion of the name, “myel,” refers to the significant white matter found in this region—especially on its exterior, which is continuous with the white matter of the spinal cord. The tegmentum of the midbrain and pons continues into the medulla because this gray matter is responsible for processing cranial nerve information. A diffuse region of gray matter throughout the brain stem, known as the reticular formation, is related to sleep and wakefulness, such as general brain activity and attention.
The Cerebellum
The cerebellum, as the name suggests, is the “little brain.” It is covered in gyri and sulci like the cerebrum, and looks like a miniature version of that part of the brain (Figure 3.10). The cerebellum is largely responsible for comparing information from the cerebrum with sensory feedback from the periphery through the spinal cord. It accounts for approximately 10 percent of the mass of the brain.
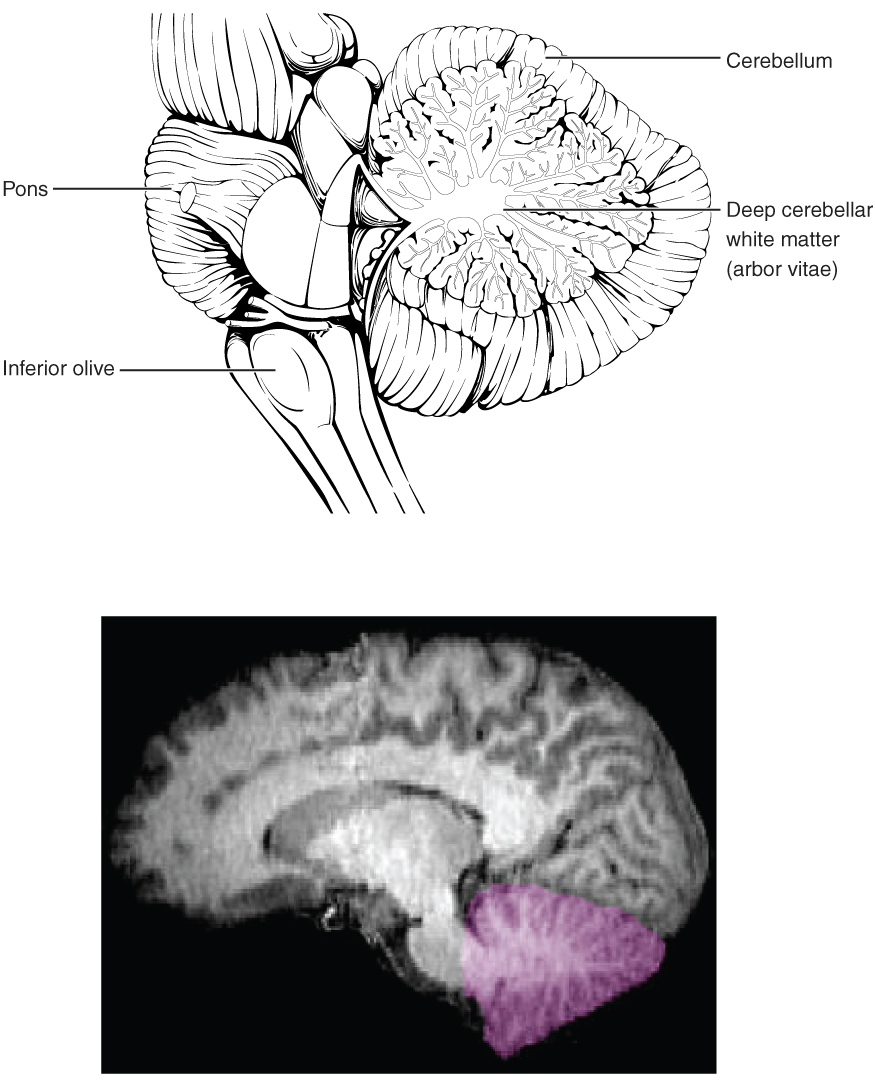
Descending fibers from the cerebrum have branches that connect to neurons in the pons. Those neurons project into the cerebellum, providing a copy of motor commands sent to the spinal cord. Sensory information from the periphery, which enters through spinal or cranial nerves, is copied to a nucleus in the medulla known as the inferior olive. Fibers from this nucleus enter the cerebellum and are compared with the descending commands from the cerebrum. If the primary motor cortex of the frontal lobe sends a command down to the spinal cord to initiate walking, a copy of that instruction is sent to the cerebellum. Sensory feedback from the muscles and joints, proprioceptive information about the movements of walking, and sensations of balance are sent to the cerebellum through the inferior olive and the cerebellum compares them. If walking is not coordinated, perhaps because the ground is uneven or a strong wind is blowing, then the cerebellum sends out a corrective command to compensate for the difference between the original cortical command and the sensory feedback. The output of the cerebellum is into the midbrain, which then sends a descending input to the spinal cord to correct the messages going to skeletal muscles.
Disorders of the…Basal Nuclei
Parkinson’s disease is a disorder of the basal nuclei, specifically of the substantia nigra, that demonstrates the effects of the direct and indirect pathways. Parkinson’s disease is the result of neurons in the substantia nigra pars compacta dying. These neurons release dopamine into the striatum. Without that modulatory influence, the basal nuclei are stuck in the indirect pathway, without the direct pathway being activated. The direct pathway is responsible for increasing cortical movement commands. The increased activity of the indirect pathway results in the hypokinetic disorder of Parkinson’s disease.
Parkinson’s disease is neurodegenerative, meaning that neurons die that cannot be replaced, so there is no cure for the disorder. Treatments for Parkinson’s disease are aimed at increasing dopamine levels in the striatum. Currently, the most common way of doing that is by providing the amino acid L-DOPA, which is a precursor to the neurotransmitter dopamine and can cross the blood-brain barrier. With levels of the precursor elevated, the remaining cells of the substantia nigra pars compacta can make more neurotransmitter and have a greater effect. Unfortunately, the patient will become less responsive to L-DOPA treatment as time progresses, and it can cause increased dopamine levels elsewhere in the brain, which are associated with psychosis or schizophrenia.